Bioequivalence Requirements
Overview
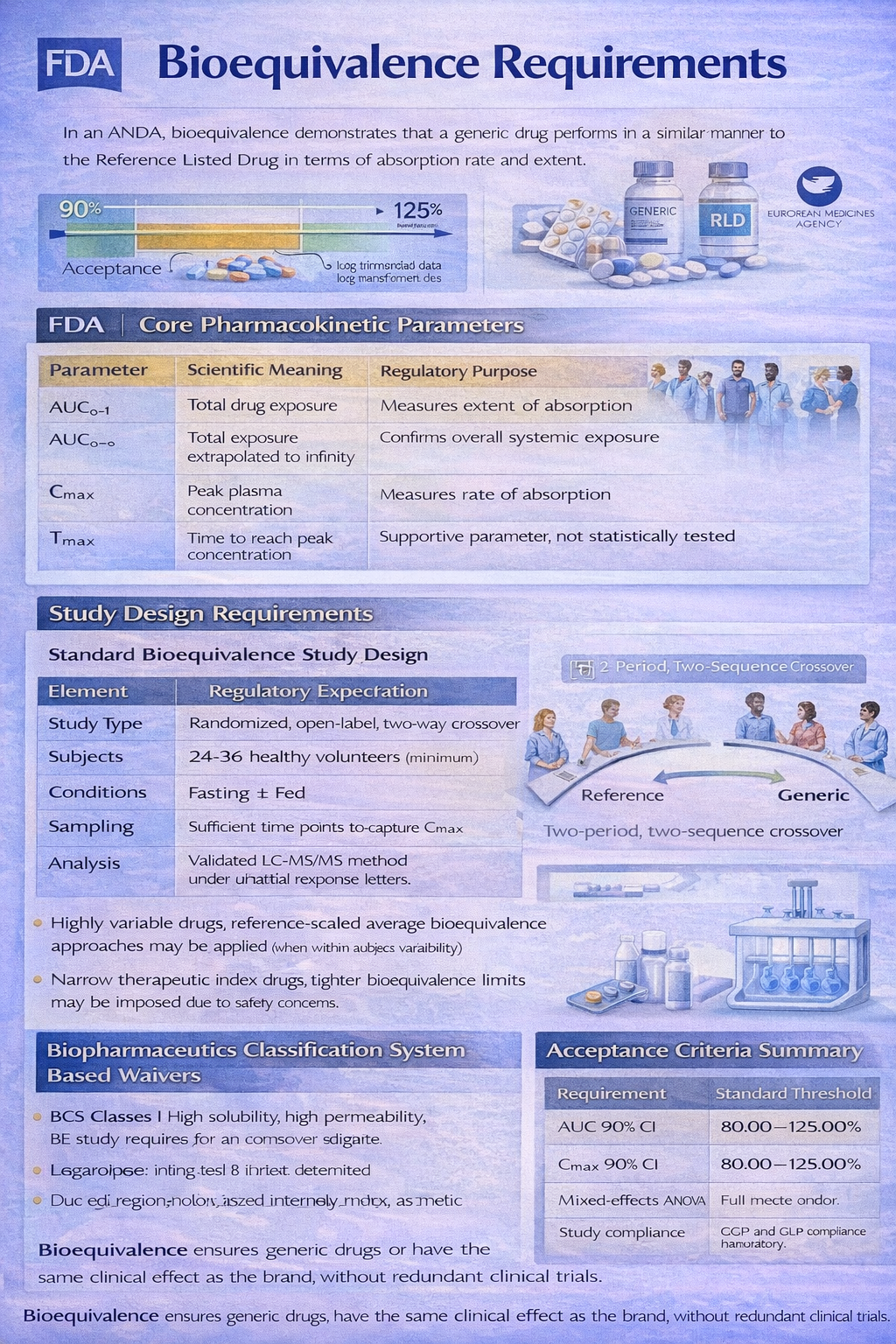
Bioequivalence Requirements form the scientific backbone of an Abbreviated New Drug Application submitted to the U.S. Food and Drug Administration under Section 505(j) of the Federal Food, Drug, and Cosmetic Act. The objective of bioequivalence is to demonstrate that the proposed generic product performs in the same manner as the Reference Listed Drug in terms of rate and extent of absorption. Unlike a New Drug Application, where full clinical efficacy and safety studies are required, an ANDA relies primarily on comparative pharmacokinetic evidence to establish therapeutic equivalence.
Bioequivalence is statistically defined through comparison of key pharmacokinetic parameters, primarily Area Under the Curve (AUC) and Maximum Plasma Concentration (Cmax). The 90 percent confidence interval of the ratio of geometric means between the test and reference product must fall within 80.00 percent to 125.00 percent. This acceptance range applies to log-transformed data and is internationally harmonized across major agencies including the European Medicines Agency.
Core Pharmacokinetic Parameters
| Parameter | Scientific Meaning | Regulatory Purpose |
|---|---|---|
| AUC0–t | Total drug exposure over time | Measures extent of absorption |
| AUC0–∞ | Total exposure extrapolated to infinity | Confirms overall systemic exposure |
| Cmax | Peak plasma concentration | Measures rate of absorption |
| Tmax | Time to reach peak concentration | Supportive parameter, not statistically tested |
Study Design Requirements
Most immediate-release oral dosage forms require a single-dose, randomized, two-period, two-sequence crossover study conducted in healthy adult volunteers under fasting conditions. In certain cases, a fed study is also required if the Reference Listed Drug labeling indicates administration with food. The washout period must be adequate, typically greater than five elimination half-lives of the drug.
Standard Bioequivalence Study Design
| Element | Regulatory Expectation |
|---|---|
| Study Type | Randomized, open-label, two-way crossover |
| Subjects | 24–36 healthy volunteers (minimum based on variability) |
| Conditions | Fasting ± Fed (if required) |
| Sampling | Sufficient time points to capture Cmax and terminal phase |
| Analysis | Validated LC-MS/MS method under GLP |
| Statistics | ANOVA on log-transformed PK parameters |
For highly variable drugs, reference-scaled average bioequivalence approaches may be applied when within-subject variability exceeds 30 percent. For narrow therapeutic index drugs, tighter bioequivalence limits may be imposed due to safety concerns.
Biopharmaceutics Classification System Based Waivers
In certain circumstances, in vivo bioequivalence studies may be waived under the Biopharmaceutics Classification System framework. BCS Class I drugs, defined as high solubility and high permeability, may qualify for a biowaiver if dissolution similarity is demonstrated across multiple pH conditions. Regulatory agencies assess dissolution profile similarity using the f2 similarity factor.
BCS Classification Overview
| BCS Class | Solubility | Permeability | BE Study Requirement |
|---|---|---|---|
| Class I | High | High | Eligible for biowaiver |
| Class II | Low | High | In vivo study required |
| Class III | High | Low | Conditional biowaiver possible |
| Class IV | Low | Low | In vivo study mandatory |
Special Dosage Forms
Modified-release products require multiple-dose steady-state studies to evaluate accumulation and fluctuation. Locally acting products such as topical dermatological preparations may require clinical endpoint studies or pharmacodynamic assessments. Inhalation products and ophthalmic products follow product-specific guidance issued by the FDA.
Regulatory Documentation in ANDA
Bioequivalence data are submitted in Module 5 of the electronic Common Technical Document format. This includes clinical study reports, analytical validation reports, subject demographics, statistical analysis plans, and raw pharmacokinetic datasets. The FDA conducts both scientific and statistical review, and may request additional data through information requests or complete response letters.
Acceptance Criteria Summary
| Requirement | Standard Threshold |
|---|---|
| AUC 90% CI | 80.00–125.00% |
| Cmax 90% CI | 80.00–125.00% |
| Statistical Model | Mixed-effects ANOVA |
| Bioanalytical Validation | Full method validation required |
| Study Compliance | GCP and GLP compliance mandatory |
Strategic Regulatory Perspective
Bioequivalence is not merely a statistical exercise but a risk-based scientific demonstration of therapeutic interchangeability. Regulatory professionals must ensure protocol alignment with FDA product-specific guidance before study initiation. Failure to design the study according to regulatory expectations can result in study rejection and significant development delay.
In conclusion, bioequivalence requirements ensure that generic medicines provide the same clinical benefit as their branded counterparts without duplicating extensive clinical trials. Mastery of study design, statistical analysis, regulatory submission standards, and agency guidance interpretation is essential for any Drug Regulatory Affairs professional working in generic drug development.
